
Vertiflex S1-S2-S3
The Vertiflex S1-S2-S3 is designed to adapt to all body shapes. Modular and customizable with various accessories, this device can be adjusted to ensure optimal comfort and efficiency.
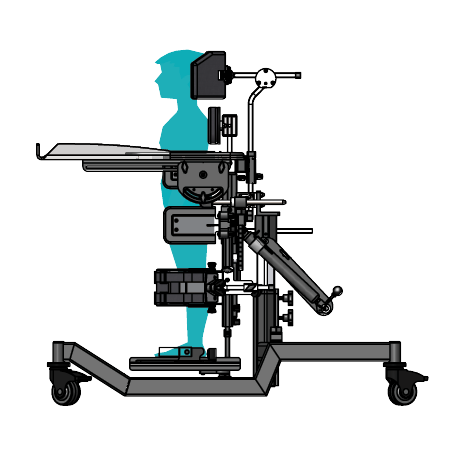
Available in 3 sizes, the Vertiflex S1-S2-S3 is a model without leg abduction. It can be configured for prone, supine or multi-positioning, and is delivered completely assembled, customized to the unique positioning needs of each child.
The cylinder assists with a full tilt from flat-to-load, making transfer easier and safer.
The upright position provides numerous benefits, both physical and psychosocial, including improved blood circulation, easier digestion, and the stimulation of muscle development.
FEATURES









SPECIFICATIONS
S1
Floor-Axilla
17-30
lbs
Base dimension
22x34
inches
Max weight
50
lbs
Colours
•••••
Possible growth
15
inches
Types
Prone
Supine
Multi-position
S2
Floor-Axilla
23-38
lbs
Base dimension
26x39
inches
Max weight
70
lbs
Colours
•••••
Possible growth
16
inches
Types
Prone
Supine
Multi-position
S3
Floor-Axilla
31-53
lbs
Base dimension
26x39
inches
Max weight
152
lbs
Colours
•••••
Possible growth
28
inches
Types
Prone
Supine
Multi-position
CHARACTERISTICS
HIGHLY MODULAR
With over 50 available accessories, the Vertiflex line can be configured for both children and adults.
EASY TILT MECHANISMS
The base unit features tilt assist for a smooth and safe transition from vertical to horizontal.
PRECISE ADJUSTMENTS
Each feature is designed for precise adjustments ensuring optimal comfort.
EASY TO USE TRAY
Our lightweight tray features a unique locking system for easy installation and removal without any knobs or clips.
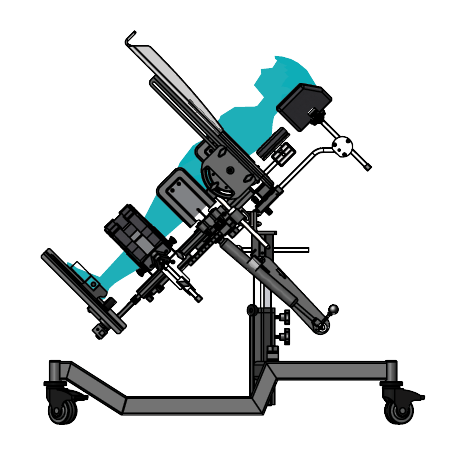
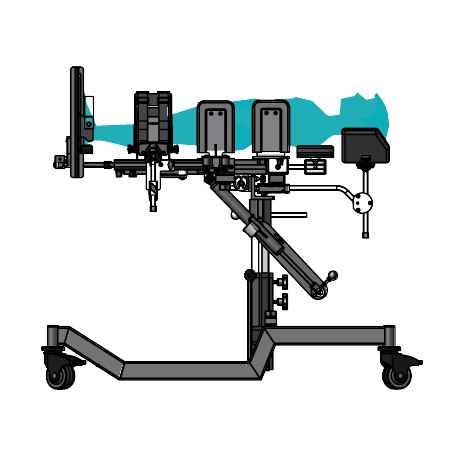
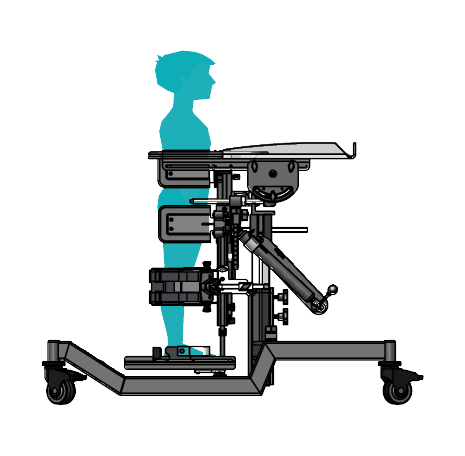
TILT POSITIONS
TECHNICAL SPECIFICATIONS
Size 1
Maximum user
weight 50 lbs
Floor to axilla measurement
17" to 30"
Growth range
15"
Base dimension
22" x 34"
Shoulder width
4" to 10"
Axillas width
5.5" to 10"
Knee width
1.5" to 3.5"
Hip width
5.5" to 10"
Size 2
Maximum user
weight 70 lbs
Floor to axilla measurement
23" to 38"
Growth range
16"
Base dimension
26" x 39"
Shoulder width
8" to 12"
Axillas width
5.5" to 14"
Knee width
2.5" to 4"
Hip width
5.5" to 14"
Size 3
Maximum user
weight 150 lbs
Floor to axilla measurement
31" to 53"
Growth range
28"
Base dimension
26" x 39"
Shoulder width
10" to 20"
Axillas width
5.5" to 18"
Knee width
2.5" to 5.5"
Hip width
5.5" to 18"
CLINICAL TIPS
Choosing the correct stander
Static standing frames are available in two configurations:
- Supine standers
- Prone standers
- Hybrid standers
Supine standers
Supine standers are those in which the child or young person is lifted or hoisted into lying on their backs. The stander is then adjusted to an appropriately more upright posture, depending on the individual’s ability. Supine standers are best for those who lack antigravity strength in the
upper trunk and neck. They can also provide a useful change of posture for those with significant hip and knee pain. While the full posterior support is useful for those with poor head and trunk control.
Prone standers
Prone standers are those in which the child or young person is tilted slightly forward. Prone standers provide anterior support requiring adequate head control in the first instance.
However, this posture is used to encourage head control, strengthen the upper trunk and shoulder girdle and inhibit extensor tone. The further the angle from upright, the less the weight bearing advantages of standing.
Hybrid standers
Hybrid standers are designed to replicate the supine and prone standers. Hybrid standers are multi and single position standers were designed to fit the widest range of children and accommodate positioning challenges few others can. Each standing frame can be configured using a wide array of accessories based on the needs of the user, the natural standing posture as far as possible.
Regardless of the stander style, the most important element is the achievement of desirable postural alignment.
What is the best angle for standing?
The more upright a person can tolerate standing, the greater the load bearing through the feet and therefore the greater the impact of the benefits of standing. There is a strong correlation between the inclination of the stander and the percentage body weight transferred and there is often large differences between right and left weight-bearing measures in the same person.
Promotes proper muscular skeleton development
Standing increases bone density and reduces the risk of fractures
Bone density is a measure of bone strength and strong bones are more resistant to fractures. Normal bone growth and development needs a combination of good nutrition, weight-bearing, and the use of muscles. Therefore children with conditions which inhibit them from doing these things lose bone density.
A more recent study assessed bone mineral loss in people with a spinal cord injury (SCI) and how weight-bearing activity (passive standing) affected this during the first two years post-injury. The Group A – those with regular physiotherapy and a standing programme (1 hour 5 days per week); and Group B – regular physiotherapy intervention.
Results indicated that after two years patients in the standing group had statistically significantly higher BMD in the legs and in the pelvis, in comparison with non-standing patients. Therefore the authors concluded that a standing programme has a statistically significant effect in the longer term on reducing the loss of bone mineral density in the lower extremities and pelvis in those with a spinal cord injury.
Decreases muscle spasms
Standing stretches muscles, preventing the apparition of new muscle pain
When children are unable to stand independently due to weakness or imbalance, they are at risk of shortening most of their muscles that are used in the hip, knee or the calf. Several researchers argue that standing provides a better position for young children to builds endurance to standing and regulate resting muscle tone.
32 research articles published from 1981 to 2008 talk about the effects of standing on motor ability and range of movement. All studies report some level of improvement regarding movement ability or increased range of movement.
Improves strength to trunk and lower extremities
Standing improves skin integrity by relieving pressure encountered during sitting
When individuals sit for lengthy periods of time, the sitting bones and the spine can become vulnerable to pressure and potential breakdown. In the standing posture, oxygenated blood can more easily reach the tissues that are usually subject to pressure. However, numerous clinical commentaries provide anecdotal evidence that standing helps to prevent painful and debilitating pressure ulcers because of improvements in circulation.
Management of atrophy in the trunk and leg muscles
Standing increases bone density and reduces the risk of fractures
Bone density is a measure of bone strength and strong bones are more resistant to fractures.
Normal bone growth and development needs a combination of good nutrition, weight-bearing, and the use of muscles. Therefore children with conditions which inhibit them from doing these things lose bone density.
A recent study evaluate the bone mineral loss in people with a spinal cord injury and how weight-bearing activity (passive standing) affected this during the first two years post-injury. The Group A – those with regular physiotherapy and a standing programme (1 hour 5 days per week); and Group B – regular physiotherapy intervention and no standing programme.
Results indicated that after two years patients in the standing group had statistically significantly higher bone mineral density in the legs and in the pelvis, in comparison with non-standing patients. Therefore they concluded that a standing programme has a statistically significant effect in the longer term on reducing the loss of bone mineral density.
Why standing is important
Human beings are designed to stand. When the development go without any complication, children start pulling themselves to a standing position from as early as nine months old. The ultimate goal is being able to move from one place to another, and achieve all the day-to-day play, self-care and school or work activities.
However, when children have severe physical disabilities (for example, cerebral palsy, spina bifida, muscular dystrophy, developmental delay, osteogenesis imperfecta or acquired injuries) which prevent them from weight bearing independently, their developmental progression may not take place. Independent standing or walking may not be achievable for some children. At this point, this is exactly why developing or maintaining an upright posture using specially designed standing frames becomes highly important.
The benefits of standing:
- Improves/maintains range of motions
- Standing and everyday activities (function)
Each physiological benefit of standing is closely related one to another, and in turn these benefits provide a wide range of psychological benefits. Those benefits can combine to improve an individual’s ability to carry out everyday activities. Many studies also prove that standing held improved the head strength, trunk and upper extremity control; improved functional reach; ability to perform fine motor tasks, hence improving enjoyment and social interaction; improved ability to work as independently as possible; increased play, physical education opportunities, even dancing; and improved ability to participate in transfers and independent dressing, resulting in self-empowerment.
Complications after stroke have been shown to impede rehabilitation, lead to poor functional outcome, and increase cost of care. This study examines the prevalence of complications related to immobility during the first year after a stroke according to functional independence and place of residence. Patients who are more independent in self-care are less at risk of complications than those who are dependent.
Posture, How it Develops, and why Standing is Important
Posture
We divide the whole body in two sections. The first one is the segments which include the head, trunk, pelvis, lower limbs and the second one is the linkages between all of them such as the spinal joints, hips, knees, ankle and shoulder joints.
Human posture is influenced by many factors:
- muscle tone (high or low)
- body shape and size (height and weight)
- gravity
- the surface
- the task in hand
Also, the posture is influence by 3 major point :
- comfort
- stability
- function (example : the ability to play, use communication devices or do schoolwork)
In the absence of stability, the function is compromise and the body can’t work correctly. However, stability can only be achieved with some degree of comfort. Function could be achieved in the absence of comfort or minimal stability, but it won’t last long. The balance must be struck between comfort, stability and function. Therefore posture is important because it supports a vast range of daily functions, in addition to supporting internal processes such as breathing, vision, digestion, circulation, temperature regulation. Humans need to be able to operate in a variety of environments, for a variety of reasons and hold themselves upright against gravity.
When not to stand?
There are very few reasons not to stand. However, those with orthopaedic or medical complications, for example, a healing fracture, severe osteoporosis, or severe hip, knee or ankle contractures may need to be excluded from a standing programme. Those with compromised breathing or circulation need to be carefully monitored when standing.
Therapists or ATP Professional?
Are you a therapist or ATP professional needing information on products or to request a product trial?
Please fill in our online request form today and we will have a Consultant reach out directly to you.
